, except for brief excerpts in connection with reviews or scholarly analysis. Use in connection with any form of information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed is forbidden. The use in this publication of trade names, trademarks, service marks, and similar terms, even if they are not identifi ed as such, is not to be taken as an expression of opinion as to whether or not they are subject to proprietary rights.
All trademarks are trademarks of their respective owners. Rather than put a trademark symbol after every occurrence of a trademarked name, we use names in an editorial fashion only, and to the benefi t of the trademark owner, with no intention of infringement of the trademark. Where such designations appear in this book, they have been printed with initial caps. McGraw-Hill eBooks are available at special quantity discounts to use as premiums and sales promotions, or for use in corporate training programs. To contact a representative please e-mail us at
F unctional MRI is a noninvasive method used to localize critical cognitive functions. Accordingly, recent interest has grown toward understanding whether fMRI-in particular, the BOLD signal-can be used to aid presurgical planning of lesion resections involving eloquent cortex to minimize disruption of cognitive function and ensure maximal tumor tissue removal. The current gold-standard method of localization is electrical cortical mapping, which, while extremely precise and predictive of postoperative deficits, is also invasive and time consuming. 30, Thus, it would be beneficial to derive fMRI-based measures that not only match the utility of electrical cortical mapping, but also help to minimize patient morbidity. Although fMRI-based mapping and electrical cortical mapping have shown varied con-Object. Functional MRI (fMRI) has the potential to be a useful presurgical planning tool to treat patients with primary brain tumor. In this study the authors retrospectively explored relationships between language-related postoperative outcomes in such patients and multiple factors, including measures estimated from task fMRI maps (proximity of lesion to functional activation area, or lesion-to-activation distance [LAD], and activation-based language lateralization, or lateralization index [LI]) used in the clinical setting for presurgical planning, as well as other factors such as patient age, patient sex, tumor grade, and tumor volume.
Abraham W, Williams J: Properties and mechanisms of LTP main tenance. Neuroscientist 2003;9:463-474.
Bloom FE: Neuroscience: From the Molecular to the Cognitive. Else vier, 1995.
Cooper JR, Bloom FE, Roth RH: The Biochemical Basis of Neuropharmacology, 8th ed. Oxford Univ Press, 2002.
Ganong WF: Review of Medical Physiology, 19th ed. Appleton & Lange, 1999.
Hille B: Ionic Channels of Excitable Membranes, 3rd ed. Sinauer, 2001. Kandel ER: The molecular biology of memory storage. Biosci Rep 2004;24:475-522.
Kandel ER, Schwartz JN, Jessell TM: Principles of Neural Science, 3rd ed. Appleton & Lange, 1991.
Levitan IB, Kaczmarek LK: The Neuron: Cell and Molecular Biology, 3rd ed. Oxford Univ Press, 2001.
Malenka RC: LTP and LTD: Dynamic and interactive processes of synaptic plasticity. Neuroscientist 1995; 1:35.
Nestler EJ, Hyman SE, Malenka RC: Molecular Neuropharmacology: A Foundation fo r Clinical Neuroscience . McGraw-Hill, 2001. Shepherd GM: The Synaptic Organization of the Brain, 4th ed. Ox ford Univ Press, 1997.
Waxman SG: Molecular Neurology. Elsevier, 2007. Waxm an SG, Kocsis JD, Stys PK (editors): The Axon: Structure, Function, and Pathophysiology. Oxford Univ Press, 1995.
Berg BO: Principles of Child Neurology. McGraw-Hill, 1996.
Bradley WG, Daroff RB, Fenichel GM, Marsden CD (editors): Neu rology in Clinical Practice, 4th ed. Butterworth-Heinemann, 2005.
Brazis PW, Masdeu JC, Biller J: Localization in Clinical Neurology. Little, Brown and Co., 2006.
Gilman S (editor): Clinical Examination of the Nervous System. McGraw-Hill, 2000.
Menkes JH, Sarnat H, Moria BL: Textbook of Child Neurology, 7th ed. Williams & Wilkins, 2005.
Binder MD (editor): Peripheral and Spinal Mechanisms in the Neural Control of Movement. Elsevier, 1999.
Brown AG: Organization in the Spinal Cord. Springer-Verlag, 1981.
Byrne TN, Benzel E, Waxman SG: Diseases of the Spine and Spinal Cord. Oxford Univ Press, 2000.
Davidoff RA (editor): Handbook of the Spinal Cord, vols 1-3. Marcel Dekker, 1984.
Kuypers HGJM: The anatomical and functional organization of the motor system. In: Scientific Basis of Clinical Neurology. Swash M, Kennard C (editors). Churchill Livingstone, 1985.
Rexed BA: Cytoarchitectonic atlas of t he spinal cord. J Comp Neurol 1954; 1 00:297.
Thach WT, Montgomery EB: Motor system. In: Neurobiology of Disease. Pearlman AL, Collins RC (editors). Oxford Univ Press, 1990.
Willis WD, Coggeshall RE: Sensory Mechanisms of the Spinal Cord, 2nd ed. Plemun, 1992.
Byrne T, Benzel E, Waxman SG: Diseases of the Spine and Spinal Cord. Oxford Univ Press, 2000. Cervical Spine Research Society: The Cervical Spine, 2nd ed. JB Lippincott, 1989.
Crock HV, Yoshizawa H: The Blood Supply of the Ve rtebral Column and Spinal Cord in Man. Springer-Ve rlag, 1977.
Newton TH, Potts DG (editors): Computed Tomography of the Spine and Spinal Cord. Clavadel Press, 1983.
Norman D, Kj os BO: MR of the spine. In: Magnetic Resonance Imaging of the Central Nervous System. Raven, 1987.
Rothman RH, Simeone FA: The Spine. WB Saunders, 1975.
White AA, Paujabi MM: Clinical Biomechanics of the Spine. JB Lippincott, 1978.
We lsh JP, Lang JP, Sugihara I, Llinas R: Dynamic organization of motor control within the olivocerebellar system. Nature 1995;374:453. REFERENCES
Bradley WG, Daroff RB, Fenichel GM, Marsden CD (editors): Neurology in Clinical Practice, 2nd ed. Butterworth Heinemann, 1996.
DeZeeuw Cl, Strata P, Voogol J (editors): The Cerebellum: From Structure to Control. Elsevier, 1998.
Foley JM: The cranial mononeuropathies. N Engl ] Med 1969; 281:905.
Hanson MR, Sweeney PJ: Disturbances of lower cranial nerves. In: Neurology in Clinical Practice, 2nd ed. Bradley WG, Daroff RB, Fenichel GM, Marsden CD (editors). Butterworth-Heinemann, 1996.
Harding AE, Deufel T (editors): The Inherited Ataxias. Raven, 1994. Horn AK, Leigh RJ: Anatomy and physiology oft he ocular motor system. Handbook Clin Ne ural. 20 11;102:21-69.
Samii M, Jannetta PJ (editors): The Cranial Nerves. Springer-Verlag, 1981.
Sears ES, Patton JG, Fernstermacher MJ: Diseases of the cranial nerves and brain stem. In: Comprehensive Neurology. Rosenberg R (editor). Raven, 1991.
Wilson-Pauwels L, Akesson EJ, Stewart PA, Spacey SD: Cranial Nerves in Health and Disease, 2nd ed. BC Decker, 2002. REFERENCES
Buijs RM, Hermes MH, Kalsbeek A: The suprachiasmatic nucleus-paraventricular nucleus interactions: A bridge to the neuroendocrine and autonomic nervous system. In: Advances in brain vasopressin. Urban LJ, Burbach JP, de Wied D. Prog Brain Res 1998;1 19:365.
Buijs RM, Kalsbeek A, Romijn HJ, Pennertz CM, Mirmiran M (edi tors): Hypothalamic Integration of Circadian Rhythms. Elsevier, 1997.
Casanueva FF, Dieguez C (editors): Recent Advances in Basic and Clinical Neuroendocrinology. Elsevier, 1989.
Ganten D, Pfaff D (editors): Morphology of Hypothalamus and Its Connections. Springer-Verlag, 1980.
Jones EG: The anatomy of sensory relay functions in the thalamus. Pages 29-53 in: Role of the Forebrain in Sensation and Behavior. Holstege E (editor). Elsevier, 1991.
Llinas R, Ribary U: Consciousness and the brain: The thalamocorti cal dialogue in health and disease. Ann NY Acad Sci 2001; 929:166-175.
Llinas RR, Steriade M: Bursting of thalamic neurons and states of vigilance. J Neurophysiol 2006;95:3297-3308.
Meijer JH, Rietveld WJ: Neurophysiology of the suprachiasmatic circadian pacemaker in rodents. Physiol Rev 1989; 89:671.
Mendoza J, Challet E: Brain clocks: From the suprachiasmatic nu cleus to a cerebral network. The Neuroscientist 2009;15: 477-488.
Purpura DP, Ya hr MD (editors): The Thalamus. Columbia Univ Press, 1986.
Renaud LP, Bourque CW: Neurophysiology and neuropharmacol ogy of hypothalamic neurons secreting vasopressin and oxytocin. Prog Neurobiol 1991;36:131.
Sherman SM, Guillery RW: Exploring the Thalamus and Its Role in Cortical Function. MIT Press, 2005.
Swaab DF, Hofman MA, Mirmiran M, Ravid R, Van Leewen F (edi tors): The Human Hypothalamus in Health and Disease . Elsevier, 1993. REFERENCES
Fishman RA: Cerebrospinal Fluid in Diseases of the Ne rvous System. WB Saunders, 1992.
Heimer L: The Human Brain and Spinal Cord. Springer-Ve rlag, 1983. Romanes GJ: Cunningham's Textbook of Anatomy, 12th ed. Oxford Univ Press, 1983.
Rosenberg GA: Brain edema and disorders of cerebrospinal fluid circulation. In: Neurology in Clinical Practice, 5th Ed. Bradley WG, Daroff RB, Fenichel GM, Jankovic J (editors). Butterworth Heinemann-Elsevier, 2008.
Seehusen DA, Reeves MM, Fomin DA: CSF analysis. Amer. Family Physician 2003;68:1103-1 108.
Sharma HS (editor): Blood-Spinal Cord and Brain Barriers in Health and Disease. Elsevier, 2004.
Wa ddington MM: Atlas of the Human Skull. Academic Books, 1983. REFERENCES
Kogure K, Hossmann KA, Siesjo B: Neurology of Ischemic Brain Damage. Elsevier, 1994.
Mohr JP, Choi D, Grotta J, Weir B, Wo lf PA: Stroke: Pathophysiology, diagnosis, and management. Lippincott, 2004.
Salamon G: Atlas of the Arteries of the Human Brain. Sandoz, 1973.
Waxman SG, Ransom BR, Stys PK: Nonsynaptic mechanisms of calcium-mediated injury in the CNS white matter. Trends Neurosci 1991;14:461.
Albin RL, Young AB, Penney JB: The functional anatomy of disor ders of the basal ganglia. Trends Neurosci 1995;200:63.
Alexander GE, deLong MR: Central mechanisms of initiation and control of movement. In: Diseases of the Nervous System: Clinical Neurobiology. Asbury A, McKhann G, McDonald WI (editors). WB Saunders, 1992.
Azizi A: And the olive said to the cerebellum. Neuroscientist 2007; 13:616-625.
Calne D, Caine SM (editors): Parkinson's Disease. Lippincott Williams & Wilkins, 2001.
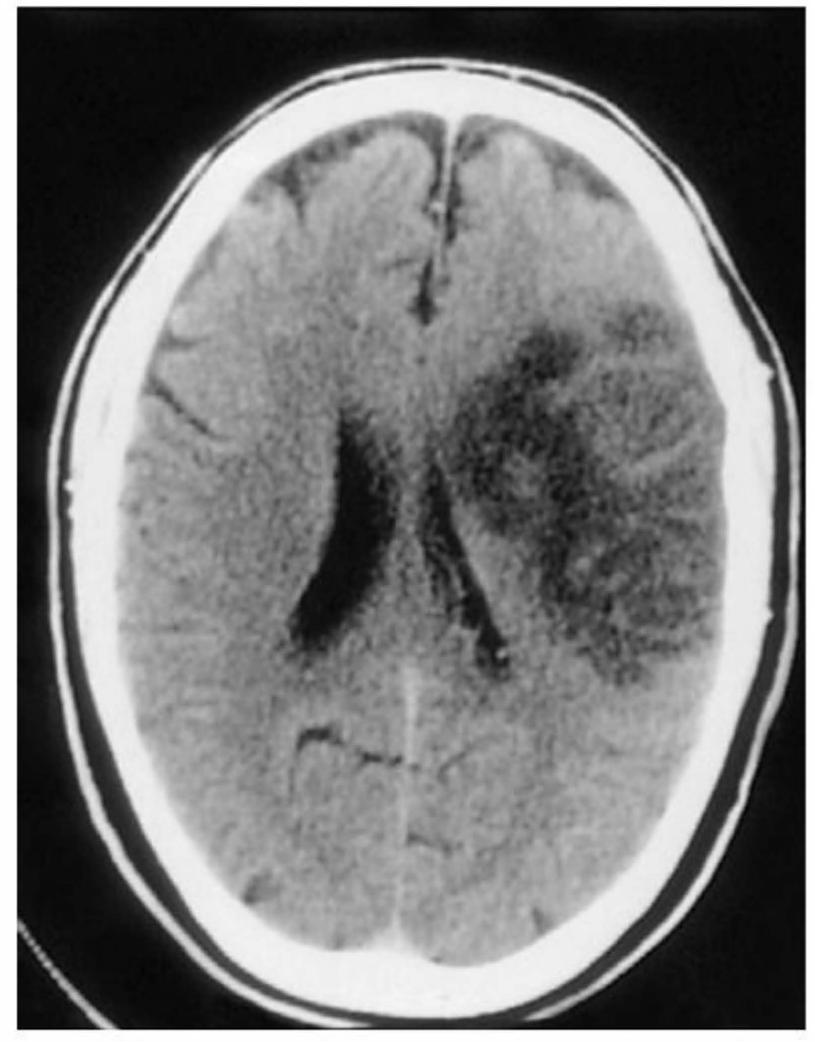
Chouinard PA, Paus T: The primary motor and premotor areas of the human cerebral cortex. Neuroscientist 2006;12:143-152. the left side of both visual fields. Complete paralysis of the left upper and lower extremities was present. Deep tendon reflexes were absent in the left upper extremity and in creased in the lower extremity. There was a left extensor plantar response, but the response was equivocal on the right. Vital signs and the complete blood count were within normal limits; blood pressure was 190/ 100. What is the preliminary diagnosis? Wo uld a lumbar puncture be indicated? Would imaging be useful? Cases are discussed further in Chapter 25.
Klein C, Krainc D, Schlossmacher MG, Larg AE: Translational research in 2010 and 2011: Movement disorders. Arch Neurol 2011;68:709-716.
Lewis JW: Cortical networks related to human use of tools. Neuro scientist 2006;12:211-23 1.
Nielson JB: How we walk: central control of muscle activity during human walking. Neuroscientist 2003;9:195-204.
Olanow CW: The scientific basis for the current treatment of Parkinson's disease. Ann Rev Med 2004;55:41-60.
Wichmann T, Vitek JL, Delong MR: Parkinson's disease and the basal ganglia: Lessons from the laboratory and from neurosurgery. Neuroscientist 1990; 1:236.
Yo ung AB: Huntington's disease: Lessons from and for molecular neuroscience. Neuroscientist 1990; 1:51.
Apkarian AV, Bushnell MC, Treede RD, Zubieta JK: Human brain mechanisms of pain perception and regulation in the health and disease. Europ J Pain 2005;9:463-484.
Borsook D, Sava S, Becerra L: The pain imaging revolution: Advancing pain into the 21st century. The Neuroscientist 2010; 16:171-185.
Devor M, Rowbotham M, Wiessenfeld-Hallin Z: Progress in Pain Research and Management. lASP Press, 2000.
Dib-Hajj SD, Cummins TR, Black JA, Waxman SG: From genes to pain. Trends Neurosci 2007;30:555-563.
McMahon S, Koltzenberg M: Wa ll and Melzack's Textbook of Pain 5th ed. Elsevier, 2011.
Snyder WD, McMahon SB: Tackling pain at the source: New ideas about nociceptors. Neuron 1998;20:629.
Alonzo JM: Neural connections and receptive field properties in the primary visual cortex. Neuroscientist 2002;8:443-456.
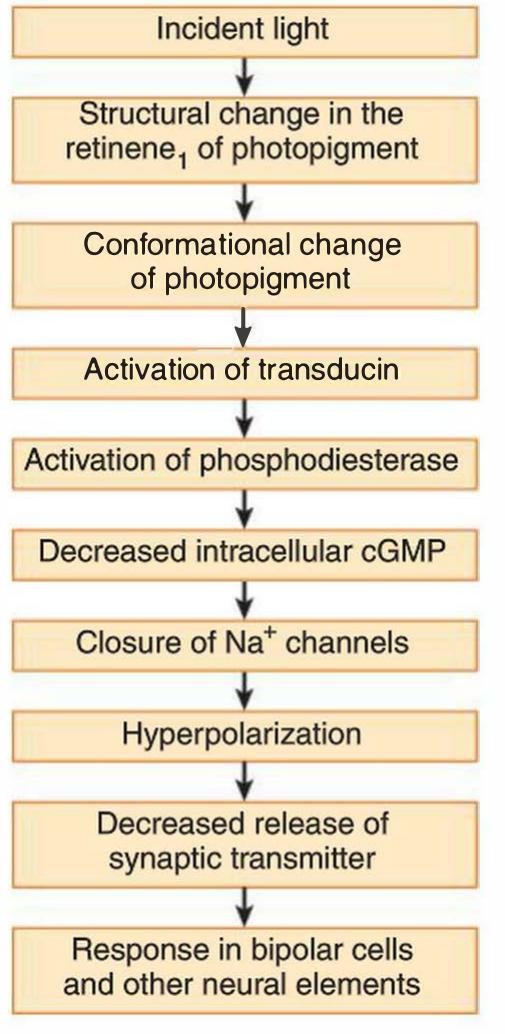
Baylor DA: Photoreceptor signals and vision. Invest Ophthalmol Vis Sci 1987;28:34.
Cohen B, Bodis-Wollner I (editors): Vi sion and the Brain. Raven, 1990. Dowling JE: The Retina: An Approachable Part of the Brain. Bell k.nap Press, Harvard Univ Press, 1987.
Gilbert CD, Li W, Piech V: Perceptual learning and adult cortical plasticity. J Physiol 2009;587:2743-2751.
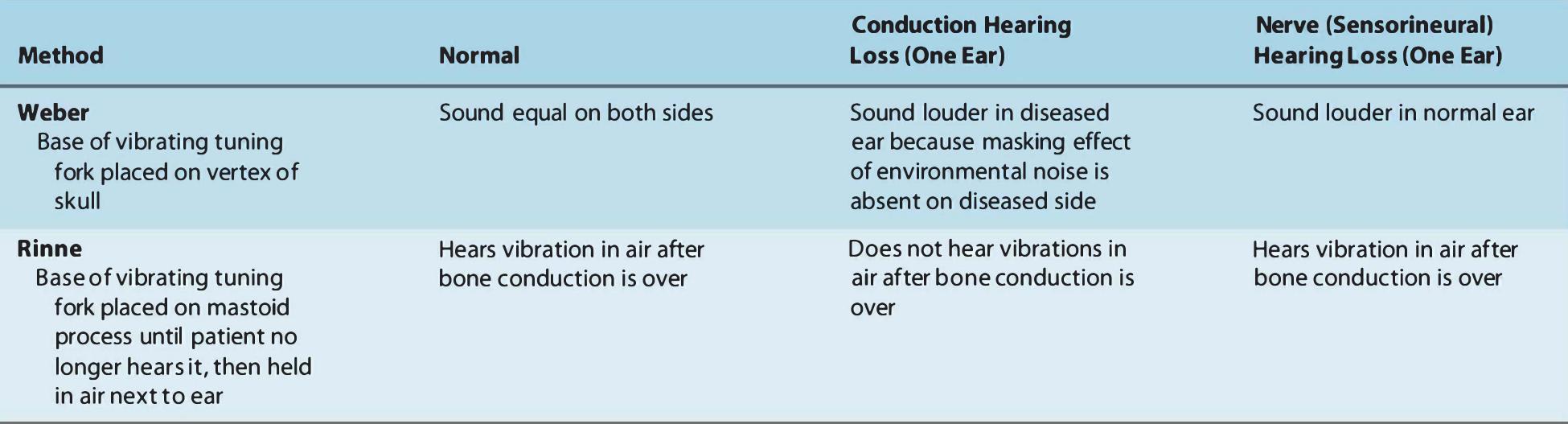
Hicks TP, Molotchnikoff S, Ono T (editors): The Vi sually Responsive Neuron: From Basic Neurophysiology to Behavior. Elsevier, 1993. REFERENCES Nerve (Sensorineural) Hearing Loss (One Earl Sound louder in normal ear Hears vibration in air after bone conduction is over
Allum JM, Allum-Mecklenburg DJ, Harris FP, Probst R (editors): Natural and Arti ficial Control of Hearing and Balance. Elsevier, 1993.
Hudspeth AJ: How hearing happens. Neuron 1997; 19:947.
Luxon LM: Disorders of hearing. Pages 434-450 in: Diseases of the Nervous System: Clinical Neurobiology, 2nd ed. Asbury AK, McKhann GM, McDonald WI (editors). WB Saunders, 1992.
Morest DK: Structural organization of the auditory pathways. Pages 19-30 in: The Nervous System, vol 3. Eagles EL (editor). Raven, 1975.
Schubert ED: Hearing: Its Function and Dysfunction. Springer Ve rlag, 1980.
Allum JH, Allum-Mecklenburg DJ, Harris FP, Probst R (editors): Natural and Artificial Control of Hearing and Balance. Elsevier, 1993.
Baloh RW, Honrubia V: Clinical Ne urophysiology of the Ve stibular System, 3rd ed. FA Davis, 2001.
Brandt T, Daroff RB: The multisensory physiological and pathologi cal vertigo syndromes. Ann Ne ural 1980;7:195.
Harada Y: The Ve stibular Organs. Kugler & Ghedini, 1988. Luxon LM: Diseases of the eighth cranial nerve. In: Peripheral Neu ropathy, 2nd ed. Dyck PJ et al (editors). WB Saunders, 1984. Pompeiano 0: Excitatory and inhibitory mechanisms in the control of posture during vestibulospinal reflexes. In: From Ne uron to Action. Deecke L, Eccles JC, Mountcastle VB (editors). Springer Ve rlag, 1992.
Borbely AA, Tobler I, Groos G: Sleep homeostasis and the circadian sleep-wake rhythm. In: Sleep Disorders: Basic and Clinical Research. MTP Press, 1983.
Crick FC, Koch C: Some reflections on visual awareness. Cold Spring Harb Symp Quant Bioi 1990;55:953.
Haider B, McCormick DA: Rapid neocortical dynamics: Cellular and network mechanisms. Neuron 2009;62: 171-189.
Jasper HH, Descarries L, Castelluci VF, Rossignol S (editors): Con sciousness: At the Frontiers of Neuroscience. Lippincott-Raven, 1998.
Koch C, Braun J: On the functional anatomy of visual awareness. Cold Spring Harb Symp Quant Biol 1996;61:49.
Kryger MH, Roth T, Dement WC: Principles and Practice of Sleep Medicine. WB Saunders, 1990.
Llinas RR, Steriade M: Bursting of thalamic neurons and states of vigilance. J Neurophysiol 2006;95:3297-3308.
Plum F, Posner JB: The Diagnosis of Stupor and Coma, 3rd ed. FA Davis, 1980.
Steriade M, McCarley RW: Brainstem Control of Wa kefulness and Sleep. Plenum, 1990.
Steriade M, McCormick DA, Sejnowski TJ: Thalamocortical oscillations in the sleeping and aroused brain. Science 1993;262:679.
Adolphs R: The human amygdala and emotion. Neuroscientist 1999;6:125.
Banasr M, Duman RS. Cell atrophy and loss in depression: reversal by antidepressant treatment Curr Opin Cell Biol 2011;23:730-738.
Bostock E, Muller RU, Kubie JL: Experience-dependent modifica tions of hippocampal place cell firing. Hippocampus 1991; 1:193.
Damasio AR: Toward a neurobiology of emotion and fe eling. Neuroscientist 1995;1:19.
Dityatev A, Bolshakov V: Amygdala, long -term potentiation, and fear conditioning. Neuroscientist 2005;11:75-88.
Koenigs M, Grafman J: Posttraumatic stress disorder: Role of the medial prefrontal cortex and amygdala. The Neuroscientist 2009;15:540-548.
Levin GR: The amygdala, the hippocampus, and emotional modula tion of memory. Neuroscientist 2004;10:31 -39.
Macguire EA, Frackowiak SJ, Frith CD: Recalling routes around London: Activation of the right hippocampus in taxi drivers. J Neurosci 1997;17:7103.
McCarthy G: Functional neuroimaging of memory. Neuroscientist 1995;1:155.
Moulton DG, Beidler LM: Structure and function in the peripheral olfactory system. Physiol Rev 1987;47: 1.
O'Keefe J, Nadel L: The Hippocampus as a Cognitive Map. Oxford Univ Press, 1978.
Reed RR: How does the nose know? Cell 1990;60:l.
Ressler KJ, Sullivan SL, Buck LB: Information coding in the olfacto ry system: Evidence for a stereotyped and highly organized epi tope map in the olfactory bulb. Cell 1994;79:1245.
Squire LR: Memory and the Brain. Oxford Univ Press, 1988. Warren-Schmidt JL, Duman RS. Hippocampal Neurogenesis: Opposing effects of stress and antidepressant treatment. Hippocampus 2006;1 6:239-249.
Zola-Morgan S, Squire LR: Neuroanatomy of memory. Ann Rev Neurosci 1993;1 6:547.
Costa M, Brookes SJ: The enteric nervous system. Am f Gastroenterol 1994;89:S129.
deGroat WC, Booth AM: Autonomic systems to the urinary blad der and sexual organs. In: Peripheral Neuropathy, 3rd ed. Dyck PJ, Thomas PK, Griffin JW et al (editors). WB Saunders, 1993.
Gershon MD: The enteric nervous system. Annu Rev Neurosci 1981;4:227.
Gibbons IL: Peripheral autonomic pathways. In: The Human Nerv ous System, 2nd ed. Paxinos G, Mai JK (editors). Elsevier Academic Press, 2004.
Goyal R, Hirano I: The enteric nervous system. N Engl J Med 1994;334: 1106.
Janig WW: The Integrative Action of the Autonomic Nervous System. Cambridge University Press, 2006.
Butefisch CM: Plasticity of the human cortex: Lessons from the hu man brain and from stroke. Neuroscientist 2004; 10:163-173.
Damasio AR, Geschwind N: The neural basis of language. Annu Rev Neurosci 1985;7:127.
Engel J, Pedley TA: Epilepsy. Lippincott-Raven, 1997. Geschwind N: The apraxias: Neural mechanisms of disorders of learned movement. Amer Sci 1975;63:188.
Goldman-Rakic P: Cellular basis of working memory. Neuron 1995;14:477.
Heilman KM, Valenstein E, Watson RT: Neglect. In: Diseases of the Nervous System, 2nd ed. Asbury AK, McKhann GM, McDonald WI (editors). WB Saunders, 1992.
Ito M (editor): Brain and Mind. Elsevier, 1997.
Kesner RP, Churchwell JC: An analysis of rat prefrontal cortex in mediating executive function. Neurobiol Learning Memory 201 1;96:471-431.
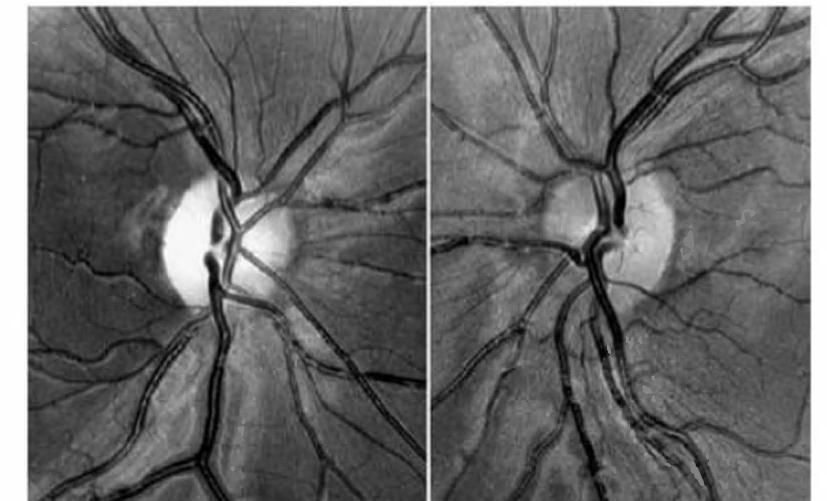
Linden DEJ: Wo rking memory networks of the human brain. Neu roscientist 2007;13:268-279. normal optic disks, but there was right hemianopsia. No other neurologic abnormality was found. Where is the lesion? What further tests would be helpful in confirming the site? What is the most likely diagnosis? Cases are discussed further in Chapter 25.
Macaluso E: Multisensory processing in sensory-specific cortical ar eas. Neuroscientist 2006;12:327-338.
Mesulam MM: Principles of Behavioral and Cognitive Neurology, 2nd ed. Oxford Univ Press, 2000.
Porter RJ: Classification of epileptic seizures and epileptic syndromes. In: A Textbook of Epilepsy. Laidlaw J, Richens A, Chadwick D (editors). Churchill Livingstone, 1993.
Posner Ml, Raichle ME: Images of Mind. WH Freeman, 1995.
Seeck M, Mainwaring M, Ives Jet al: Differential neural activity in the human temporal lobe evoked by fa ces of family members and friends. Ann Neurol 1993;34:369.
Shaywitz BA, Shaywitz SE, Pugh KR et al: Sex differences in the functional organization of the brain fo r language. Nature 1995;373:607.
Springer SP, Deutch G: Left Brain, Right Brain. WH Freeman, 1987.
Tsao DY, Livingstone MS: Mechanisms of face perception. Ann Rev Neurosci 2008;31:411-43 1.
Superior sagittal sinus
Inferior sagittal sinus
Internal cerebral vein
Basal vein of Rosenthal 8. Frontal ascending vein
Rolandic vein of Tro lard 10. Parietal ascending vein 11. Communicating temporal vein of Labbe 12. Descending temporo-occipital vein REFERENCES
Cabeza R, Kingstone A (editors): Handbook of Functional Neuroimaging of Cognition. MIT Press, 2006.
Chugani H: Metabolic imaging: A window on brain development and plasticity. Neuroscientist 1999;5:29.
Damasio H: Human Brain Anatomy in Computerized Images. Oxford Univ Press, 1995.
Detre JA, Floyd TF: Functional MRI and its application in clinical neuroscience. Neuroscientist 2002;7:64.
Greenberg JO: Neuroimaging. McGraw-Hill, 1999.
Kaplan RT, Atlas SW: Pocket Atlas of Cranial Magnetic Resonance Imaging. Lippincott Williams & Wilkins, 2001.
Mills CM, deGroot J, Posin JP: Magnetic Resonance Imaging: Atlas of the Head, Neck, and Spine. Lea & Febiger, 1988.
Oldendorf WH: The Quest fo r an Image of the Brain. Raven, 1980.
Osborn AG: Introduction to Cerebral Angiography. Harper & Row, 1980.
Senda M, Kimura Y, Herscovitch P (editors): Brain Imaging using PET. Elsevier, 2002.
Tamraz JC, Comair Y, Luders HO: Atlas of Regional Anatomy of the Brain using MRI. Oxford, 2000.
To ga A, Mazziotta J (editors): Brain Mapping: The Systems. Elsevier, 2000.
Toga A, Mazziotta J, Frackowiak R: Brain Mapping: The Disorders. Elsevier, 2000.
Truwit CL, Lempert TE: High Resolution Atlas of Cranial Neuroanatomy. Williams & Wilkins, 1995.
Wa rach S: Seeing tl!e brain so we can save it: Magnetic resonance imaging as a clinical tool. In: From Neuroscience to Neurology, Waxman SG (editor). Elsevier Academic, 2005. REFERENCES
American EEG Society: Guidelines in EEG and evoked potentials. l Clin Neurophysiol 1986;3(Supp 1):1.
Neurotransmitters found in the brain stem include- 1. acetylcholine
Norepinephrine is found in the- 1. sympathetic nervous trunk 2. locus ceruleus 3. lateral tegmentum of the midbrain 4. neuromuscular junction 22. Glutamate- !. is the transmitter at the neuromuscular junction 2. may be involved in excitotoxicity 3. is a major inhibitory transmitter in the CNS 4. is a major excitatory transmitter in the CNS 23. Decussations are- 1. aggregates of tracts 2. fiber bundles in a spinal nerve 3. horizontal connections crossing within the CNS from the dominant to nondominant side
vertical connections crossing within the CNS from left to right or vice versa
Inhibitory transmitters in the CNS include- 1. glutamate (presynaptic inhibition)
GABA (presynaptic inhibition)
GABA (postsynaptic inhibition)
The neurotransmitter dopamine- !. is produced by neurons that project from the sub stantia nigra to the caudate and putamen
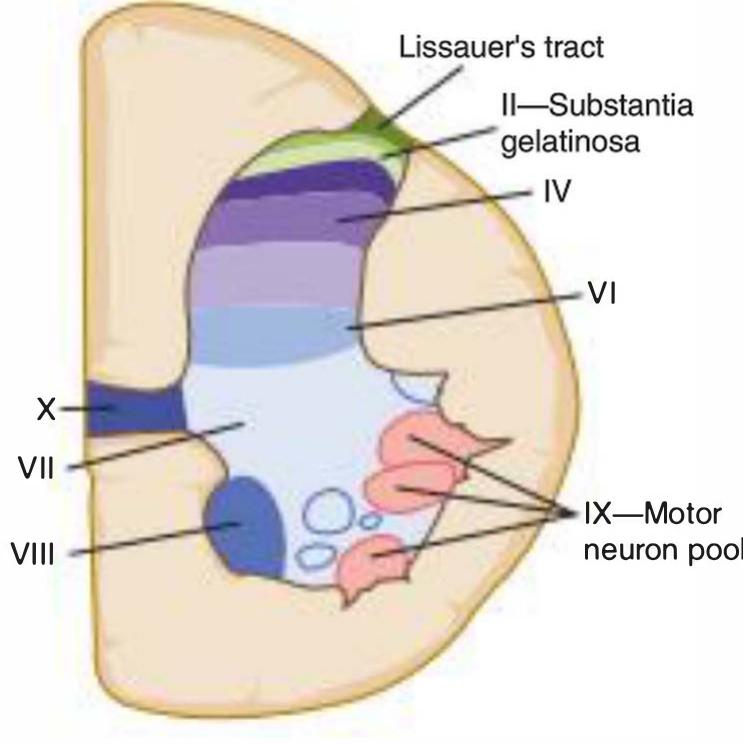
Fine-diameter dorsal root axons of LS on one side termi- nate in the- 1. marginal layer of the ipsilateral dorsal horn 2. ipsilateral substantia gelatinosa 3. ipsilateral lamina V of the dorsal horn 4. ipsilateral dorsal nucleus (of Clarke)
Axons in the spinothalamic tract- 1. carry information about pain and temperature (lat eral spinothalamic tract) and light touch (anterior spinothalamic tract)
carry information about pain (lateral spinothalamic tract) and temperature (anterior spinothalamic tract)
decussate within the spinal cord, within one or two segments of their origin
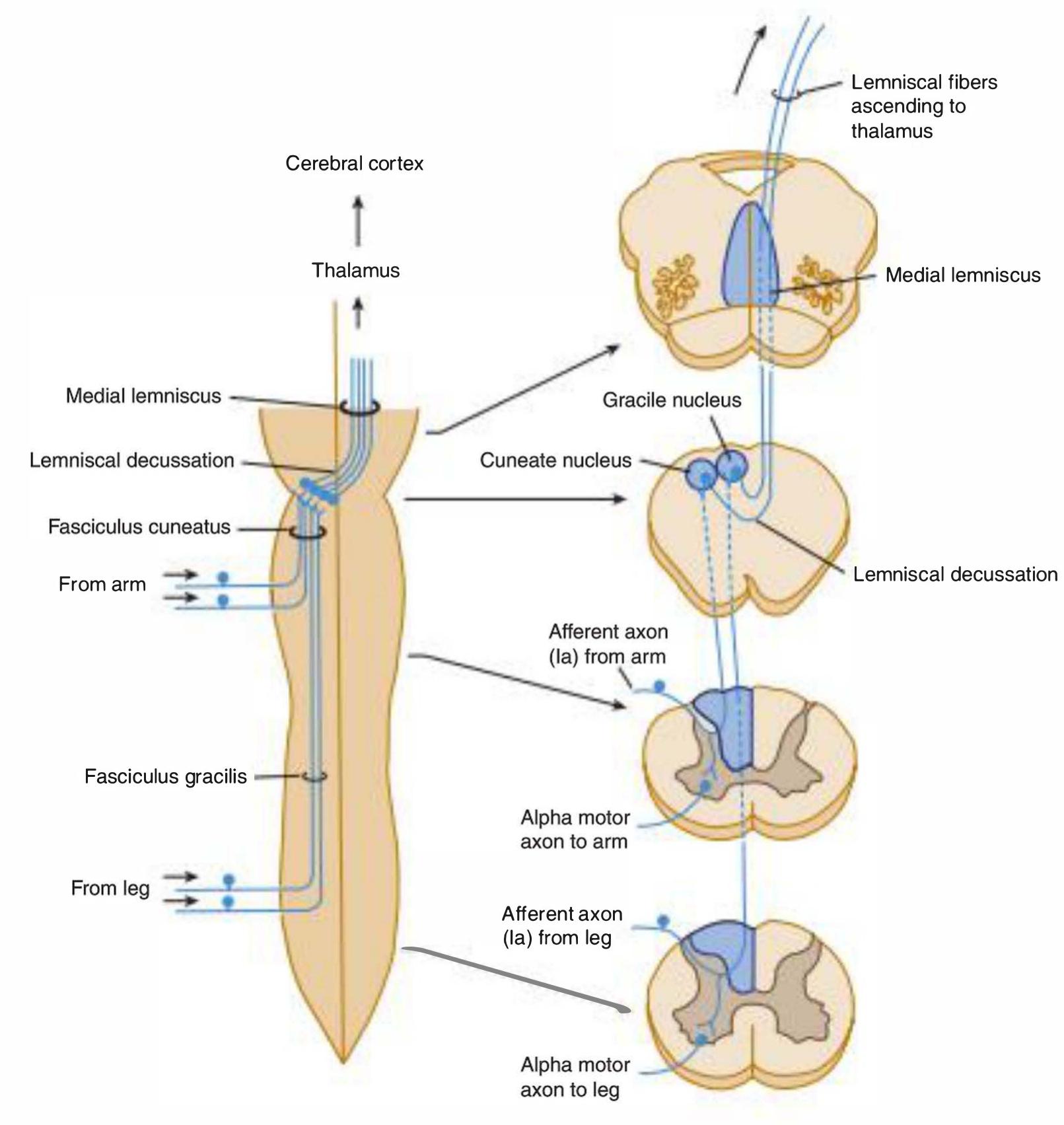
synapse in the gracile and cuneate nuclei 11. The dorsal spinocerebellar tract- 1. arises in the dorsal nucleus of Clarke and, above C8, in the accessory cuneate nucleus
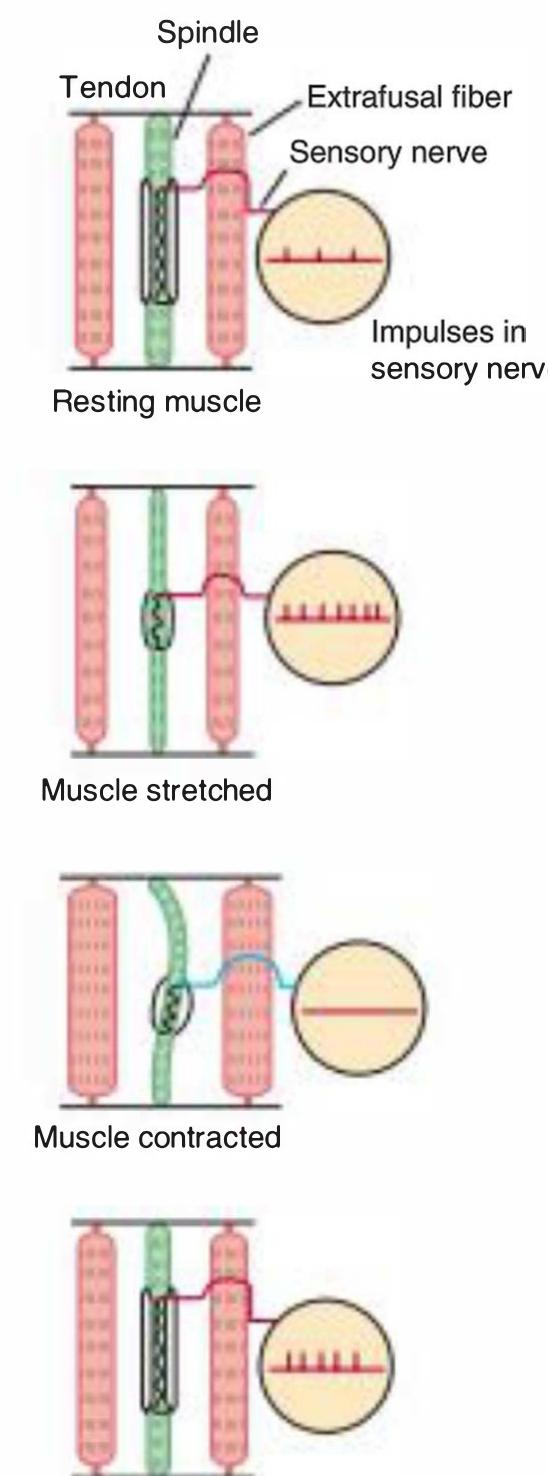
carries information arising in the muscle spindles, Golgi tendon organs, touch and pressure receptors
projects without synapses to the basal ganglia and cerebellum
Second-order neurons in the dorsal column system- 1. convey information about pain and temperature 2. cross within the lemniscal decussation 3. cross within the pyramidal decussation 4. convey well-localized sensations of fm e touch, vi bration, two-point discrimination, and propriocep tion 13. The fo llowing rules about dermatomes are correct- 1. the C4 and T2 dermatomes are contiguous over the anterior trunk
the thumb, middle fm ger, and 5th digit are within the C6, C7, and C8 dermatomes, respectively
Signs of upper-motor-neuron lesions include- 1. Babinski's sign 2. hypoactive deep tendon reflexes and hyporetlexia 3. spastic paralysis 4. severe muscle atrophy
A-delta and C peripheral afferent fibers- 1. terminate in laminas I and II of the dorsal horn 2. convey the sensation of pain 3. terminate in lamina V of the dorsal horn 4. convey the sensation of light touch
Cortical area 17- 1. is also termed the striate cortex 2. is involved in the processing of auditory stimuli 3. receives input from the lateral geniculate body 4. receives input from the medial geniculate body 14. Within the cerebellum- !. climbing fibers and mossy fibers carry afferent in fo rmation
Purkinje cells provide the primary output from the cerebellar cortex
Purkinje cells project to the ipsilateral deep cerebel lar nuclei
efferents from the deep cerebellar nuclei project to the contralateral red nucleus and thalamic nuclei 15. In a patient with a missile wound involving the left cerebral hemisphere, the fo llowing might be expected- 1. dense neglect of stimuli on the left side 2. hemiplegia involving the right arm and leg 3. hemiplegia involving the left arm and leg 4. aphasia
Auditory stimuli normally cause impulses to pass through the-
The principal neurotransmitter(s) released by synaptic terminals of sympathetic axons is/are- 1. epinephrine 2. norepinephrine 3. acetylcholine
Alzheimer's disease is characterized by- 1. neurofibrillary tangles 2. loss of neurons in the basal fo rebrain (Meynert) nucleus
severe pathology in CA1
Destruction of the lower cervical and upper thoracic ventral roots on the left side leads to- 1. dilated right pupil 2. constricted right pupil 3. dilated left pupil 4. constricted left pupil 15. After transection of the peripheral nerve, the- 1. axons and Schwarm cells distal to the cut undergo degeneration and disappear
sensory axons distal to the cut survive, but motor axons degenerate
motor neurons whose axons were cut degenerate and disappear
surviving axons of the proximal stump will send out new growth cones to attempt regeneration 16. The Kliiver-Bucy syndrome- 1. is characterized by hyperorality and hypersexuality 2. is characterized by psychic blindness and personal ity changes
is seen in patients with lesions of the anterior thala mus 17. Pain sensation- !. is carried in large myelinated (A-alpha) axons 2. is carried by small myelinated and unmyelinated (A-delta and C) axons
is carried upward in the spinothalamic tract and spinoreticulothalamic system
Parasympathetic fibers are carried in- 1. cranial nerves III and VII 2. cranial nerves IX and X 3. sacral roots S2-4
the lateral and anterior columns of the spinal cord
D 9. A 14. B 19. c 24. c 23. The homunculus in the motor cortex- 5. B 10. B 15. A 20. E 25. c 1. contains magnified representations of the fa ce and hand 2. represents the fa ce highest on the convexity of the Section IV hemisphere
The optic chiasm- 1. is located close to the pineal and is often com- Section V pressed by pineal tumors 2. is located close to the pituitary and is often com-
 Ale Rmz
Ale Rmz




























![FIGURE 2-16 Main changes that take place in an injured nerve fiber. A: Normal nerve fiber, with its perikaryon and the effector cell (striated skeletal muscle). Notice the position of the neuron nucleus and the amount and distribution of Nissl bodies. B: When the fiber is injured, the neuronal nucleus moves to the cell periphery, Niss] bodies become greatly reduced in number (chromatolysis), and the nerve fiber distal to the injury degenerates along with its myelin sheath. Debris is phagocytized by macrophages. C: The muscle fiber shows pronounced disuse atrophy. Schwann cells proliferate, forming a compact cord that is penetrated by the growing axon. The axon grows at a rate of 0.5 to 3 mm/d. D: In this example, the nerve fiber regeneration was successful, and the muscle fiber was also regenerated after receiving nerve stimuli. E: When the axon does not penetrate the cord of Schwann cells, its growth is not organized and successful regenera tion does not occur. (Redrawn and reproduced, with permission, from Willis RA, Willis AT: The Principles of Pathology and Bacteriology, 3rd ed. Butterworth, 1972.)](https://figures.academia-assets.com/35806578/figure_027.jpg)



























































































![FIGURE 7-14 Magnetic resonance image showing, in the sagittal plane, a mass lesion (arrow heads) in the patien described in Case Illustration 7-3. The mass lesion, which was shown on biopsy to be a germinoma, compressed the quadrigeminal plate and obstructed the cerebral aqueduct [arrow]. (Case illustration and image courtesy of Joachim Baehring, MD, Yale University School of Medicine.) This tragic case illustrates the locked-in syndrome. The in- farction, in the base of the pons, destroyed the corticospinal and corticobulbar tracts and thus produced paralysis of the limbs and bulbar musculature. Preservation of the oculomotor and trochlear nuclei and of their nerves permitted some](https://figures.academia-assets.com/35806578/figure_112.jpg)
































































































![FIGURE 11-19 An81-year-old woman was admitted with shortness of breath and fever. She was found to have a right middle lobe pneumonia, the third pneumonia in three months. Neurologic examination r evealed a vocal cord paralysis on the right side; the gag reflex was absent and there was loss of bulk of the trapezius and sternocleidomastoid muscles on the right side; the t ongue appeared slightly atrophic o1 the right and deviated to the right upon protrusion; there was asymmetric elevation of the soft palate (deviation to the left due to paralysis on the right side). The patient aspirated during a swallowing evaluation. Magnetic resonance imaging of the brain demonstrated amass lesion within the jugular foramen and the petrous bone on the right side [left image, arrow heads]. Computed t omography of the base of the skull showed osteolytic changes within the right petrous temporal and occipital bone [right: arrow heads; asterisk: jugular foramen]. A biopsy confirmed the clinically suspected diagnosis of glomus jugulare tumor which had impaired function of the ninth, t enth, eleventh and twelfth cranial nerves. The patient was treated with radiation. (Courtesy of Dr. Joachim Baehring.)](https://figures.academia-assets.com/35806578/figure_201.jpg)























































![FIGURE 15-3 Neural components of the retina. C, cone; R, rod; MB, RB, FB, bipolar cells (of the midget, rod, and flat types, respectively); DG and MG, ganglion cells (of the diffuse and midget types, respectively); H, horizontal cells; A, amacrine cells. (Reproduced, with permission from Dowling JE, Boycott BB: Organization of the primate retina: Electron microscopy. ProcRoy Soc Lond Ser B [Biol] 1966;166:80.)](https://figures.academia-assets.com/35806578/figure_251.jpg)











![FIGURE 15-18 Activation of visual cortex as shown by functional magnetic resonance imaging (fMRI). A: An oblique axial anatomic MRI. The region showing increased activity in response to a full-field patterned stimulus has been assessed by fMRI (using a method known as echoplanar MRI) and is shown in white. B: Activation of the visual cortex on the left side in response to patterned visual stimulation of the right visual hemifield (black) and activation of the right-sided visual cortex in response to patterned stimulation of the left hemifield. The changes in signal intensity are the result of changes in flow, volume, and oxygenation of the blood in response to the stimuli. (Data from Masuoka LK, Anderson AW, Gore JC, McCarthy G, Novotny EJ: Activation of visual cortex in occipital lobe epilepsy using functional magnetic r esonance imaging. Epilepsia 1994;35[Supp 8]:86.) “ As visual information is relayed from cell to cell in the primary visual cortex, it is processed in increasingly complex](https://figures.academia-assets.com/35806578/figure_265.jpg)













































































![The CT scanning apparatus rotates a narrow x-ray beam around the head. The quantity of x-ray absorbed in small vol- umes (voxels [volume elements, or units]) of brain, measuring approximately 0.5 mm? x 1.5 mm or more in length, is com- puted. The amount of x-ray absorbed in any slice of the head can be thus determined and depicted in various ways as pixels](https://figures.academia-assets.com/35806578/figure_337.jpg)