Zivile Pranskuniene
Zivile Pranskuniene
580 California St., Suite 400
San Francisco, CA, 94104
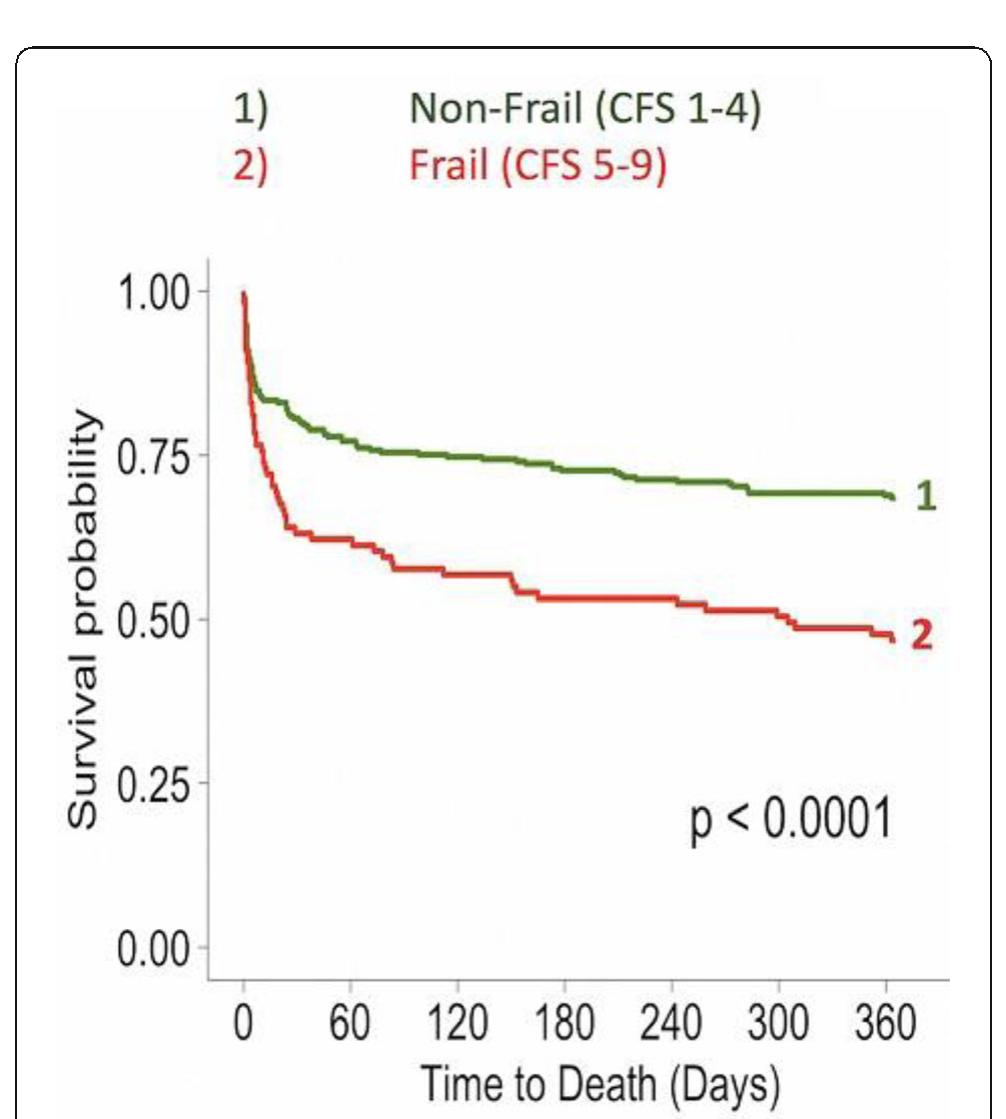
Introduction: The purpose of the study was to determine whether the preferential localization of the infection and age affect the prognostic value of the genetic marker AQP5 (1364A/C, rs3759129) in outcome prediction in sepsis patients. Studies by Adamzik and colleagues have demonstrated that aquaporin AQP5 polymorphism (1364A/C, rs3759129) associates with increased 30-day survival in sepsis patients presumably due to increased gene expression that enhance the leukocyte migration. To increase the informative value of the prediction and decrease the cost, it might be crucial to determine at a pre-test level the subset of patients who might benefit most from the prognostic genotyping. Methods: Sepsis and septic shock were defined in patients according to SEPSIS-3 (2016) recommendations. Study groups (n=152) included ICU patients with abdominal sepsis (AS, including pancreatitits, peritonitis, cholecystitis, appendicitis; n=98) and sepsis patients with other sources of infections. AQP5 polymorphism was studied by analyzing PCR products in a 2% agarose gel using a AQP5 1364A/C specific tetra primer set. Data were analyzed by Kaplan-Meyer plot and Fisher test, and odds ratios were calculated. Results: Distribution of alleles (A and C) and genotypes (AA, CA and CC) AQP5 1364A/C in patients with sepsis or sepsis subgroups (sepsis with no septic shock and sepsis shock patients) versus control group (healthy volunteers) did not differ. Although there was a trend to preferential survival of sepsis patients with genotype C AQP5 despite the source of infection, only patients with AQP5 CC or CA genotype and abdominal sepsis (Sepsis-3), or a subgroup of the same AQP5 genotype experiencing septic shock, demonstrated increased 30-day survival versus AA homozygotic patients (P<0.002). Conclusions: The informative value of detecting the AQP5 CC or CA genotype for prognosis of 30-day survival versus AA homozygotic patients is increased only in abdominal sepsis patients.











![Table 1 (abstract P014). Multivariate analysis for evaluating the risk of organ failure based on the LCN2 expression levels. Adjusting variables were [age], [chronic cardiac disease], [cancer], [immunosuppression], [hypertension], [chronic respiratory disease], [chronic renal failure], [respiratory focus], [abdomen focus]](https://figures.academia-assets.com/110459643/table_005.jpg)

![Table 2 (abstract P014). Multivariate analysis for evaluating the risk of mortality based on the LCN2 expression levels. Adjusting variables were [age], [chronic renal failure], [diabetes], [respiratory focus]](https://figures.academia-assets.com/110459643/figure_009.jpg)
















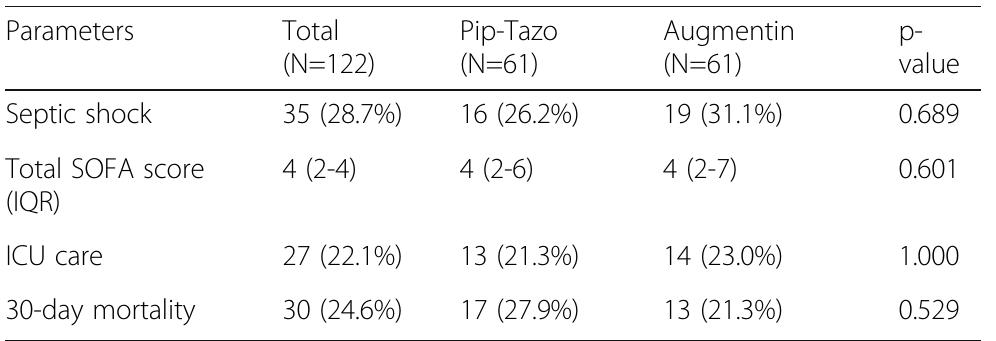
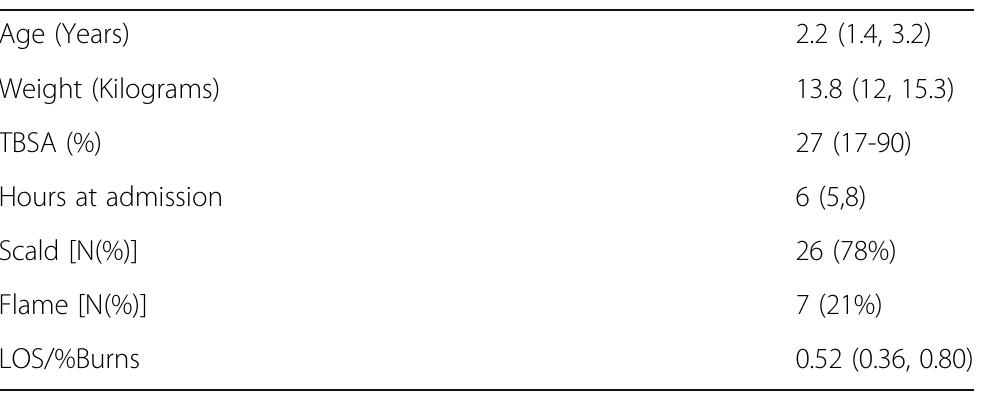
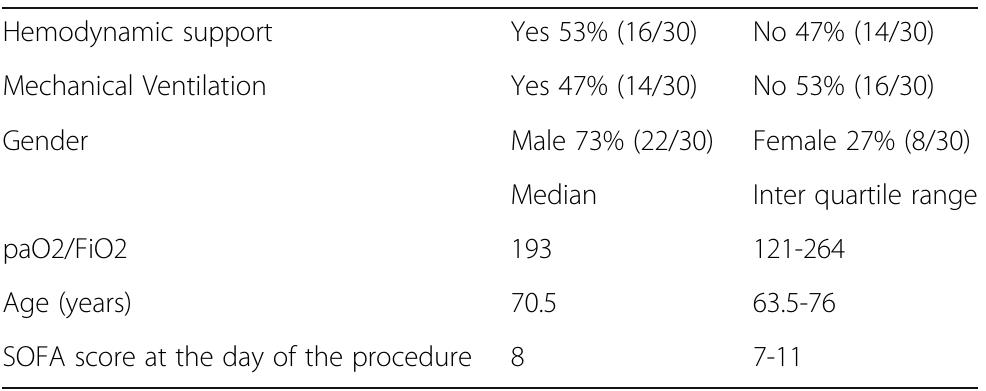
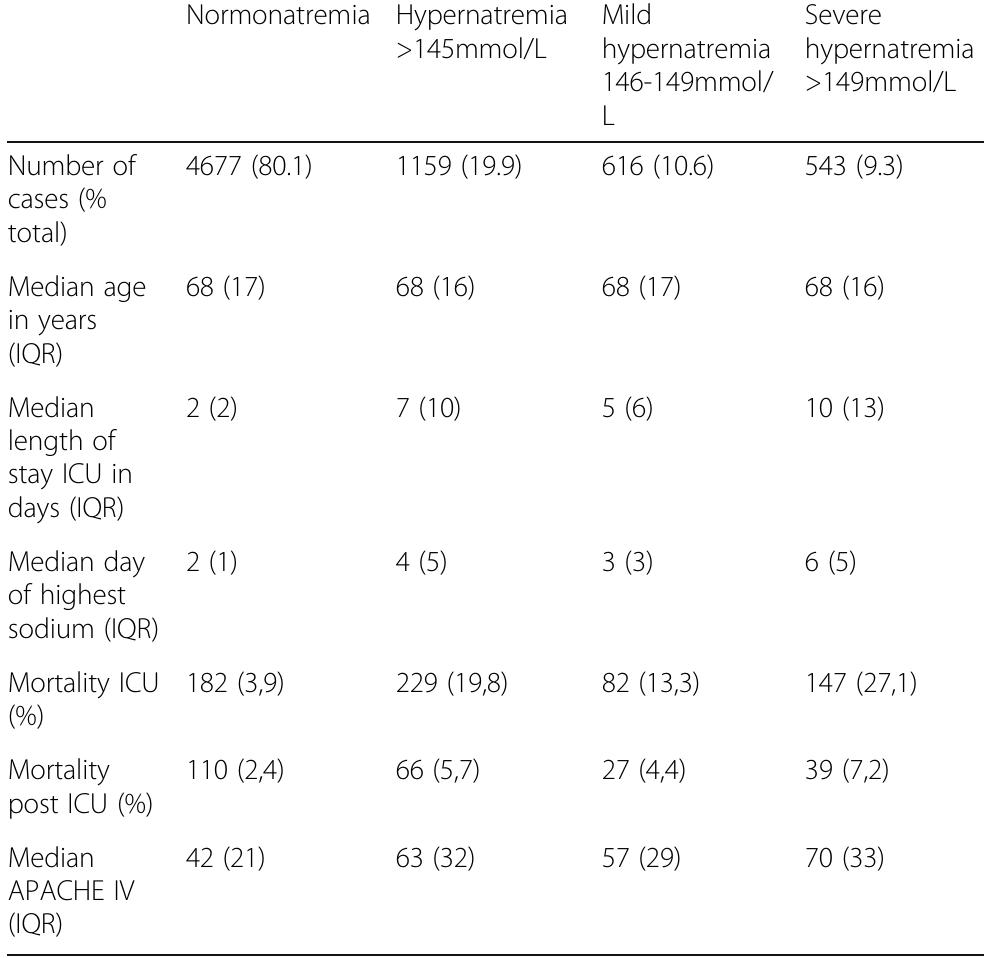
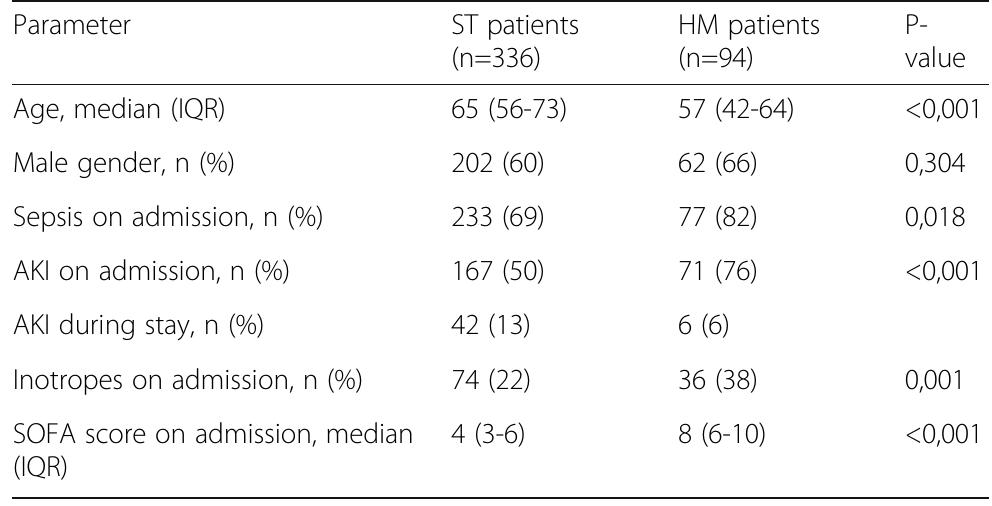
![Table 1 (abstract P036). See text for description Data presented as number (percentage) and median [interquartile range] Table 2 (abstract P036). See text for description](https://figures.academia-assets.com/110459643/table_011.jpg)



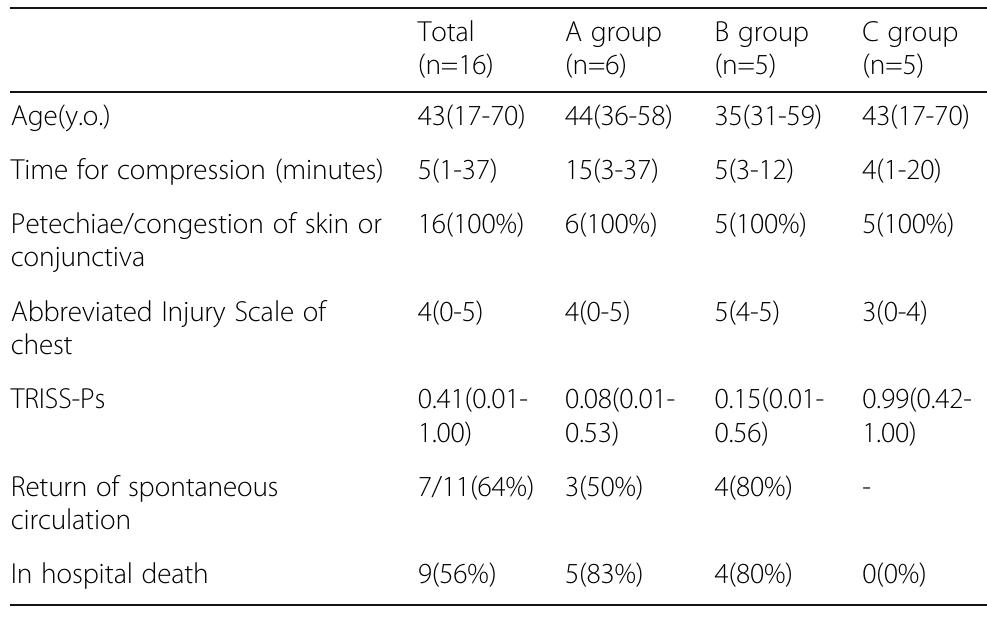
![Data presented as number (percentage) and median [interquartile range]](https://figures.academia-assets.com/110459643/figure_023.jpg)





















































































































![Fig. 1 (abstract P204). Median (inter-quartile range) regional cerebral oxygen saturation (rSO2) in patients with good (Cerebral Performance Category [CPC] 1-2) and poor (CPC 3-5) neurological outcome during the first 36 h after intensive care unit (ICU) admission](https://figures.academia-assets.com/110459643/figure_099.jpg)
![Fig. 1 (abstract P205). Scatter plots of serum neuron-specific enolase (NSE) concentration at 48 h after cardiac arrest vs. median regional cerebral oxygen saturation (rSO2) during the first 36 h in intensive care unit in patients with good (Cerebral Performance Category [CPC] 1-2) and poor (CPC 3-5) neurological outcome Conclusions: We did not find any association between cerebral oxy- genation during the first 36 h of post-resuscitation intensive care and NSE serum concentrations at 48 h after cardiac arrest. Results: We did not find significant correlation between median rSOz and serum NSE concentration at 48 h after cardiac arrest, rs = -0.08, p = 0.392 (Figure 1). The median (IQR) NSE concentration at 48 h was 17.5 (13.4-25.0) ug/l and 35.2 (22.6-95.8) g/l in patients with good and poor outcome, respectively, p < 0.001.](https://figures.academia-assets.com/110459643/figure_100.jpg)























![{1] Czosnyka M et al. J. Neurosurg., 88:802-808, 1998 Reference](https://figures.academia-assets.com/110459643/figure_115.jpg)








































![Fig. 1 (abstract P2839). Serial creatinine results pre-and post ECMO [1] Antonucci E et al. Artificial Organs 40:746-54, 2016. {2] Forni LG et al. Intensive Care Med 43:855-866, 2017. P290B P290A References](https://figures.academia-assets.com/110459643/figure_140.jpg)









































![[1] Reminiac et al. JAMPDD. 2016; 29(2):134-41. Reference](https://figures.academia-assets.com/110459643/figure_174.jpg)































































![[1] Hudson D et al. Int J Med Informatics 112, 131-136, 2018 Reference](https://figures.academia-assets.com/110459643/figure_215.jpg)









![Fig. 1 (abstract P445). Hierarchy of intervention effectiveness [from 1]](https://figures.academia-assets.com/110459643/figure_224.jpg)