ASHRAF ALQUDWA
ASHRAF ALQUDWA
580 California St., Suite 400
San Francisco, CA, 94104
AI
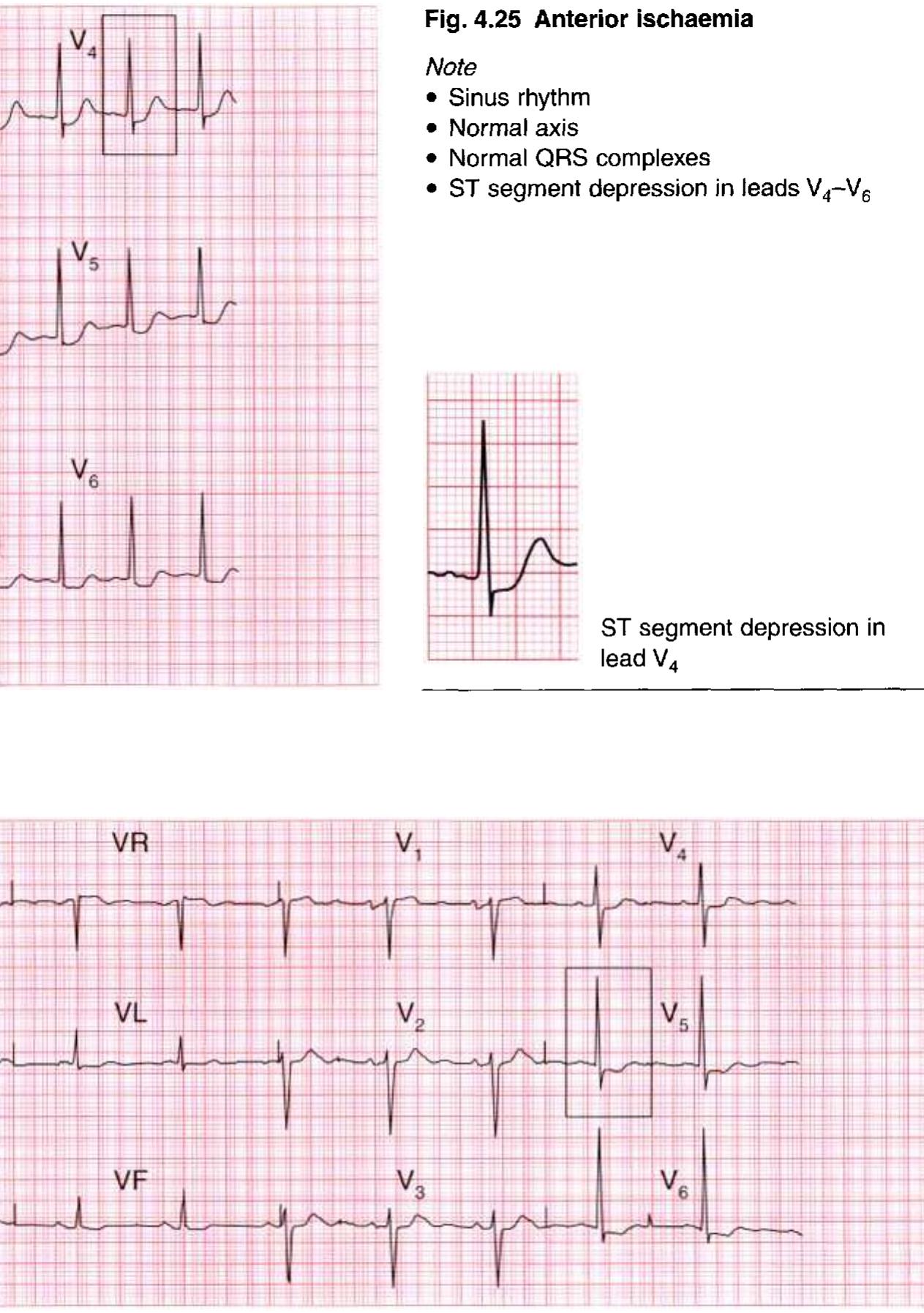
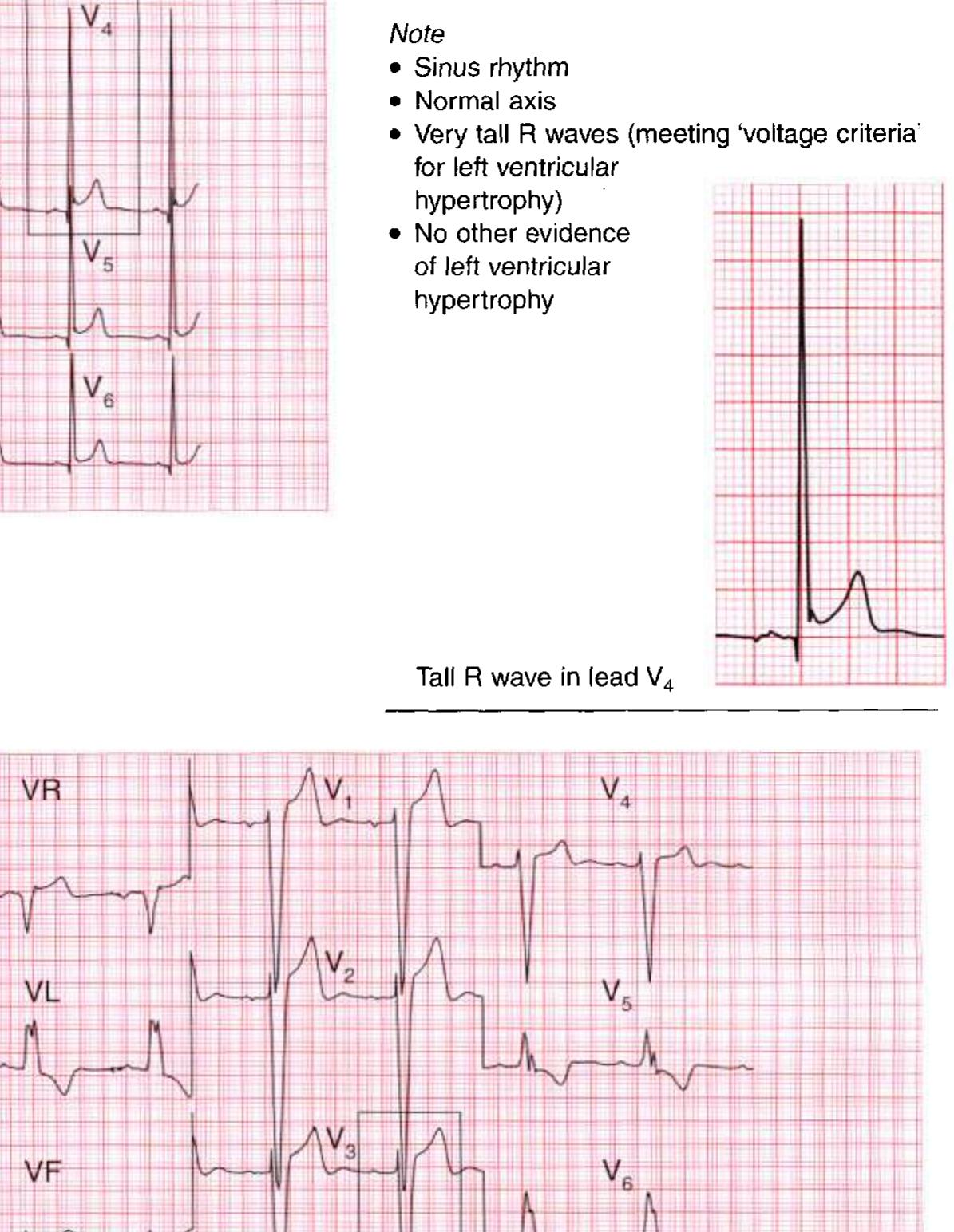
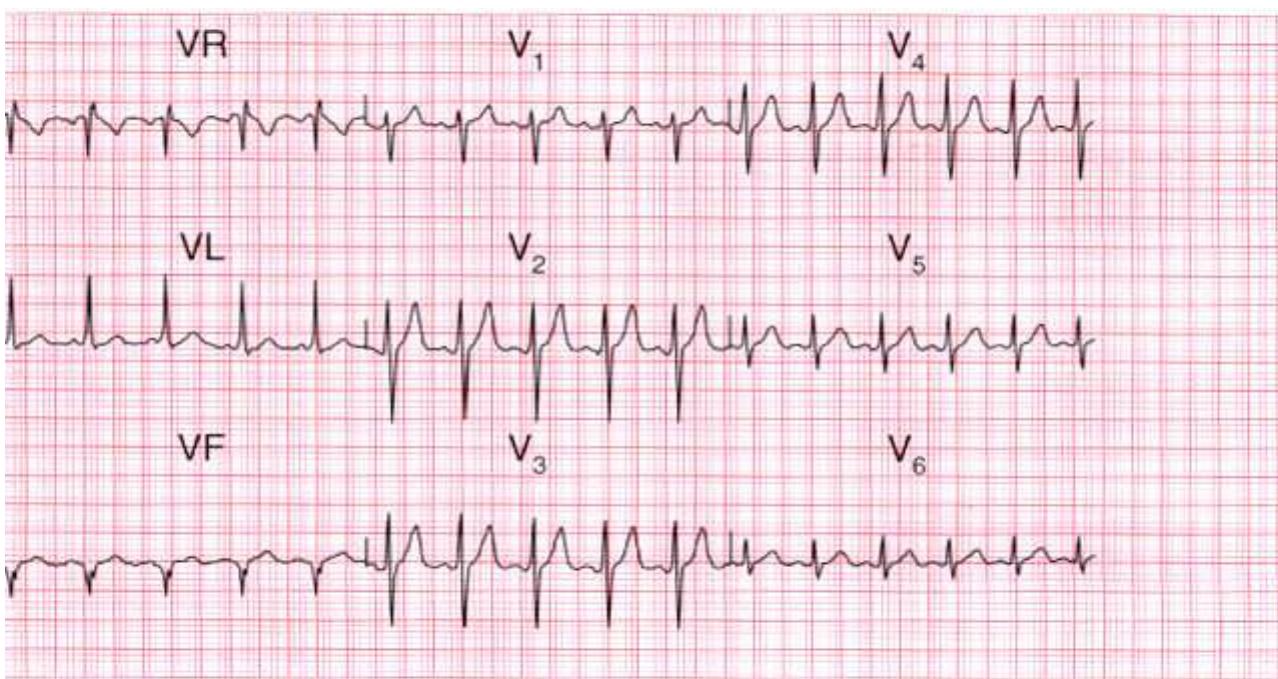
The paper discusses the critical interpretation of electrocardiograms (ECGs) in clinical practice, highlighting common ECG abnormalities and their clinical correlations. It emphasizes that a normal ECG does not necessarily rule out heart disease, and conversely, abnormal ECG patterns can appear in healthy individuals. The paper details various conditions associated with specific ECG findings, serving as a comprehensive guide for practitioners in accurately diagnosing and distinguishing cardiac conditions.
















































































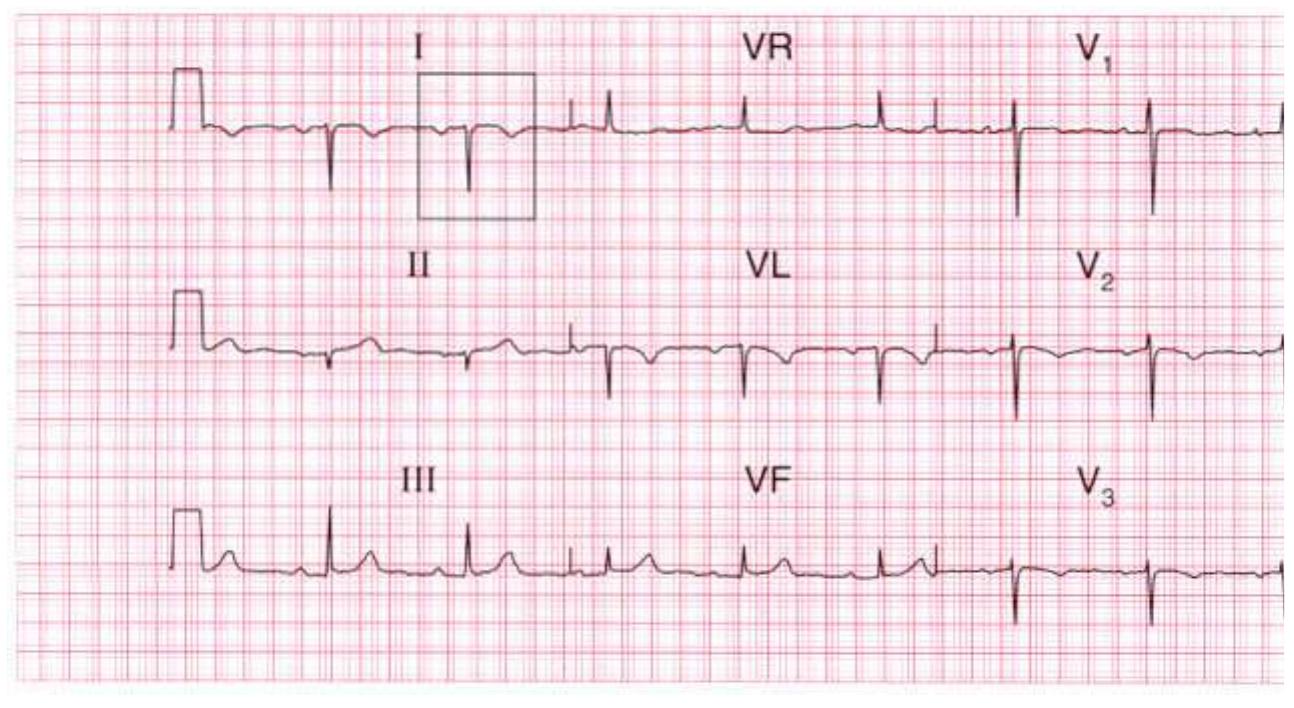










































































































































































































































































































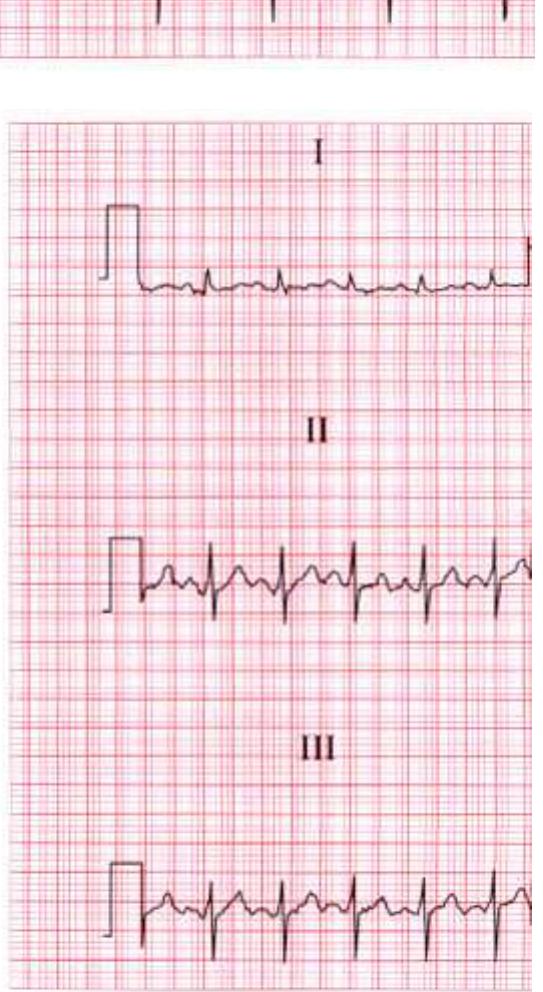
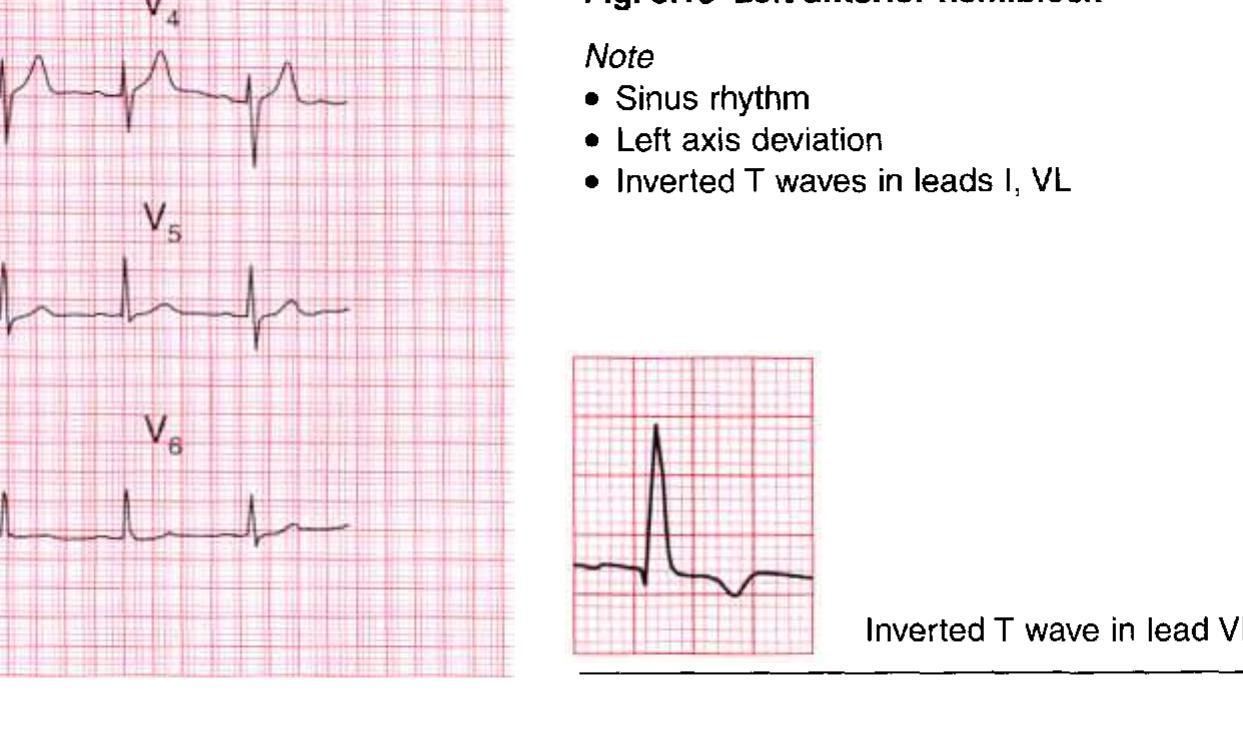
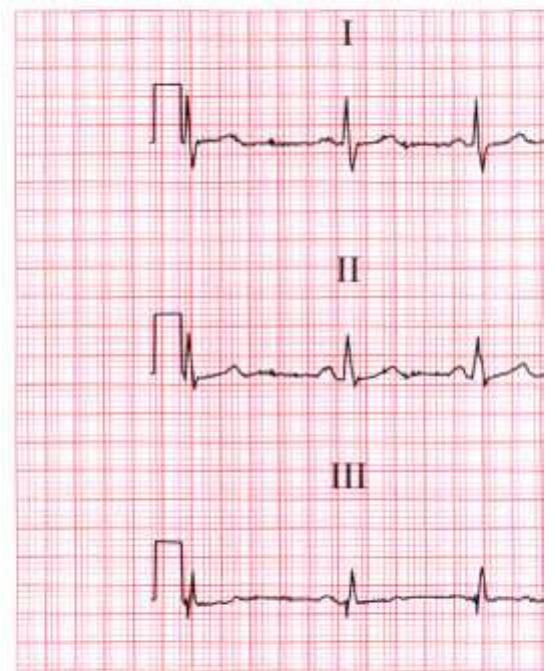
![S waves in jeads J] and Ill: left axis deviation](https://figures.academia-assets.com/36721212/figure_392.jpg)